Decoding Malaria: The Tiny Enemy Inside Your Red Blood Cells.

Malaria, also known as “ague” or marsh fever, is an infectious disease that remains a major global public health problem, particularly in tropical and subtropical regions. The World Health Organization (WHO) estimates that in 2024 there were roughly 263–282 million malaria cases worldwide and about 600,000 deaths, most of them in children under 5 years of age. In Southeast Asia, including Thailand, the disease is still found in forested and border areas. Rapid and accurate diagnosis is therefore central to treatment and disease control.
This article provides a systematic overview of the malaria parasite — from the species and life cycle, to symptoms and species identification, through to laboratory diagnostic methods and the use of rapid tests for screening in real-world settings.
1. What Is Malaria and What Causes It
Malaria is caused by protozoan parasites of the genus Plasmodium, with the female Anopheles mosquito as the disease vector. When an infected mosquito bites a person, the parasite in the sporozoite stage enters the bloodstream and first develops in the liver, then emerges to invade and destroy red blood cells, producing the symptoms of the disease.
Transmission Routes
Most often transmitted through the bite of an infected female Anopheles mosquito
May also be transmitted via blood transfusion, sharing needles, and from mother to child during pregnancy
Not transmitted from person to person through ordinary contact
2. How Many Species of Malaria Are There
There are 5 main Plasmodium species that cause disease in humans (some sources count P. ovale as 2 subspecies — P. ovale curtisi and P. ovale wallikeri — bringing the total to 6). The 2 species posing the greatest threat are P. falciparum and P. vivax.
| Species | Key features / severity | Fever pattern | Distribution / notes |
| P. falciparum | The most severe and dangerous; the leading cause of death; can progress to severe illness within 24 hrs | Fever every ~48 hrs (malignant tertian); often without a clear rhythm | Most prevalent in Africa; also found in Asia/Thailand |
| P. vivax | The most widely distributed; has a dormant “hypnozoite” stage in the liver, causing relapse | Fever every ~48 hrs (benign tertian) | Predominant in Asia and Latin America; common in Thailand |
| P. malariae | Symptoms usually mild, but can persist in the body for many years | Fever every ~72 hrs (quartan) | Found sporadically throughout the tropics |
| P. ovale | Symptoms usually mild; has a dormant liver stage and can relapse (curtisi / wallikeri) | Fever every ~48 hrs (benign tertian) | Most common in West Africa |
| P. knowlesi | Primarily from monkeys; multiplies rapidly; can become severe | Fever daily ~24 hrs (quotidian) | Found in Southeast Asia, especially Malaysia and forested areas |
What Laboratories Must Watch For
P. knowlesi resembles P. malariae (mature stage) and P. falciparum (ring stage) under the microscope, so it can be misdiagnosed.
Correct species identification directly affects drug selection and prognosis.
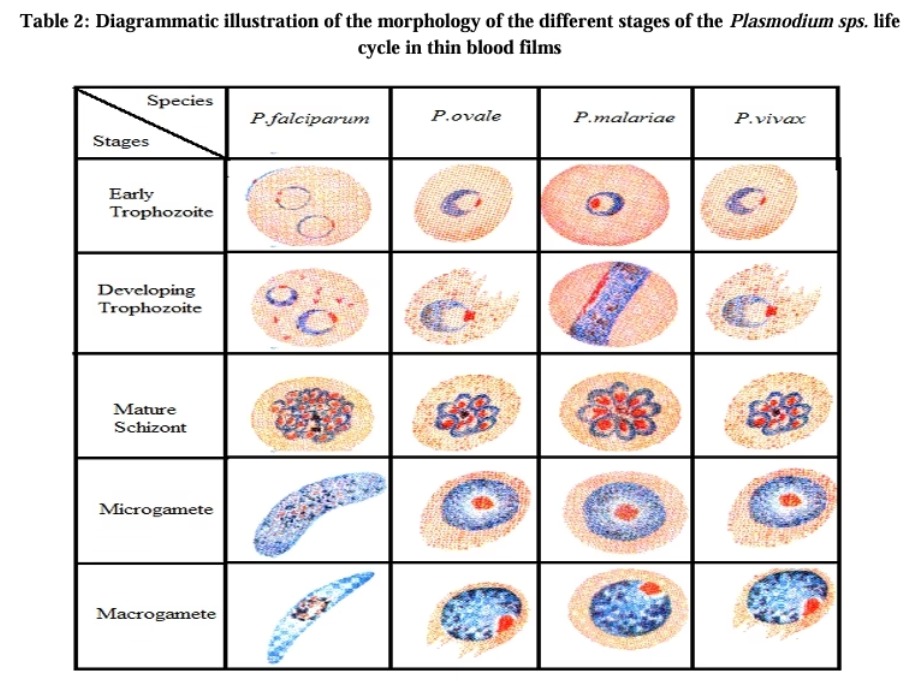
3. Life Cycle and Blood Stages of the Parasite (How Many Forms)
After leaving the liver and entering red blood cells, the parasite develops through various stages visible on a blood film — the basis for both “species identification” and “staging the parasite.” These are generally divided into 4 main stages:
- Ring stage (Ring / immature trophozoite) — the earliest stage, ring-shaped; at this stage all species look very similar, making identification by eye difficult
- Trophozoite stage — the parasite matures further and shows malarial pigment; differences between species become clearer
- Schizont (dividing) stage — the parasite divides into multiple merozoites within the red blood cell before the cell ruptures and releases parasites to infect new cells
- Gametocyte (sexual) stage — the reproductive stage taken up by mosquitoes for transmission; in P. falciparum it has a distinctive banana or crescent shape
Ref: https://alliedguru.com/determination-of-malaria-parasites/
Key Insight
In P. falciparum, usually only ring stages and gametocytes are seen in peripheral blood, because mature stages adhere to blood-vessel walls; finding multiple stages or multiply-infected red cells is therefore a clue to this species
P. vivax and P. ovale have a dormant “hypnozoite” stage in the liver, allowing the disease to relapse even after the bloodstream infection has cleared
4. Clinical Features of Malaria
Early symptoms are often nonspecific, resembling a cold or general fever, making diagnosis difficult if malaria is not considered. The incubation period is generally about 7–30 days after a mosquito bite. Common symptoms include:
- Fever, chills, and sweating, which may occur in cycles (the malaria paroxysm cycle)
- Headache, muscle aches, and fatigue
- Nausea, vomiting, abdominal pain, and diarrhea
- Anemia from red-cell destruction, and an enlarged liver/spleen
Severe symptoms (common in P. falciparum):
- Drowsiness, confusion, seizures, or unconsciousness (cerebral malaria)
- Difficulty breathing and respiratory failure
- Kidney failure, jaundice, low blood sugar, and severe anemia
Warning
If left untreated, P. falciparum malaria can progress to severe illness and death within 24 hours. Rapid diagnosis is therefore very important.

5. How to Differentiate / Identify the Species
“Differentiation” has two main levels: (1) determining whether it is malaria at all, and (2) determining which species. Identification can be done through several approaches:
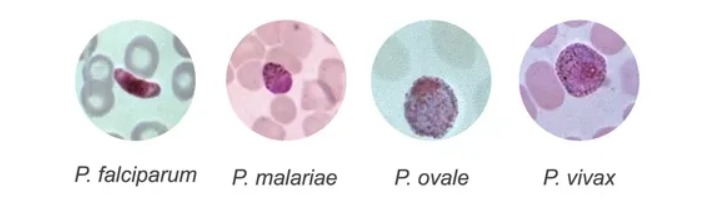
5.1 Morphological identification under the microscope
A long-standing standard method that relies on differences in parasite shape at each stage and on changes in the infected red blood cells. Criteria used to distinguish species include:
- Size of the infected red blood cell (enlarged or normal); e.g., P. vivax/P. ovale tend to enlarge the red cell
- Dots or granules within the red cell, e.g., Schüffner’s dots in P. vivax/P. ovale
- Number of merozoites in the schizont stage, and the shape of gametocytes (e.g., banana shape in P. falciparum)
- Presence of multiple stages simultaneously, or multiply-infected red cells
5.2 Antigen-based identification
Rapid tests detect antigens specific to the parasite.
5.3 Molecular identification
PCR and real-time PCR can identify species with the greatest accuracy, detect low parasite levels, and help confirm cases that are difficult to identify by microscopy or rapid test, such as P. knowlesi.
6. Laboratory Diagnosis
WHO recommends that all suspected malaria cases be confirmed by parasite-based diagnosis before treatment is started. The main methods used in the laboratory are:
| Method | Advantages | Limitations |
| Microscopy (Giemsa-stained smear) — reference standard | Can identify species, can quantify parasitaemia, low cost | Requires expertise and time to read; sensitivity depends on examiner skill; not ideal for urgent field work |
| Rapid test | Results in 15–20 minutes; easy to perform without complex equipment; suitable for screening and field use | Cannot quantify parasites; may remain positive after cure (HRP2); reduced sensitivity at low parasite levels |
| PCR / Molecular | Highest sensitivity and specificity; detects low parasite levels and identifies species accurately | High cost; requires specialized equipment and personnel; takes longer |
| Serology (antibody testing) | Indicates past infection; suitable for epidemiology and blood-donor screening | Not suitable for diagnosing acute infection |
7. Can Screening Be Done with a Rapid Test?, and How Does It Work?
The answer is “yes.” Rapid tests are a malaria screening tool accepted by WHO and used widely around the world, especially in areas where microscopy is hard to access. Rapid tests use the principle of immunochromatography (lateral flow) to detect parasite antigens from just a few drops of blood, with results available within 15–20 minutes.
Antigens Used in Testing
- HRP2 (Histidine-Rich Protein 2): an antigen specific to P. falciparum — highly sensitive for this species
- pLDH (Plasmodium Lactate Dehydrogenase): available as pan-pLDH found across multiple species and as species-specific forms; notable for clearing quickly after the parasite is eliminated, thus reflecting an active infection
- Aldolase: a pan-specific shared antigen found in all malaria species; used in some products
Malaria Pf/Pan Test Kit — A Fast and Accurate Screening Option
NS Promedica is pleased to introduce the Malaria Pf/Pan Test Kit, a rapid immunochromatographic test that detects antigens to distinguish between P. falciparum (Pf) and other malaria species (Pan) in a single test. It is suitable for screening in hospitals, clinics, mobile units, and remote areas.

Malaria Pf/Pan test (Cassette) – NS Promedica
Advantages of the Malaria Pf/Pan Test Kit
| Highlight | Benefit to the user |
| Rapid results | Results in about 15–20 minutes, helping clinicians decide on treatment quickly and reducing the risk of severe disease |
| Preliminary differentiation (Pf vs Pan) | Indicates whether it is P. falciparum (the most dangerous) or another species, helping plan appropriate treatment |
| Easy to use | Requires only a few drops of blood and no complex equipment; suitable for staff at various levels and for field work |
| Sensitivity–specificity meeting standards | Designed to meet standard thresholds for screening, reducing both false negatives and false positives |
| Suitable for resource-limited settings | No need for a microscope or electricity; easy to store and carry; suitable for border/forest areas |
| Supports high-volume screening | Helps screen at-risk patients quickly in a single run, improving disease-surveillance efficiency |
Conclusion
Malaria remains a disease requiring vigilance — especially P. falciparum, which is severe and can be rapidly fatal. Accurate and timely diagnosis is the key. Microscopy remains the reference standard, while the Pf/Pan rapid test fills the gap in speed and accessibility, enabling faster patient screening and timely referral for treatment.
The Malaria Pf/Pan Test Kit is therefore an option that meets the needs for speed, convenience, and preliminary species differentiation, suitable for screening across a variety of situations. Used together with confirmatory testing as appropriate, it helps raise the standard of patient care and malaria control effectively.
Academic references: WHO Fact Sheet & World Malaria Report 2024–2025, CDC DPDx, the Merck Manual, and the Malaria Journal